Sacrum
| Sacrum | |
|---|---|
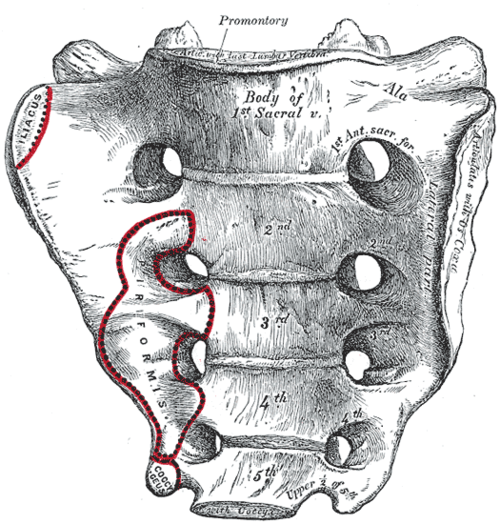 Sacrum, pelvic surface | |
 Image of a male pelvis (sacrum is in center) | |
| Details | |
| Identifiers | |
| Latin | Os sacrum |
| MeSH | D012447 |
| TA98 | A02.2.05.001 |
| TA2 | 1071 |
| FMA | 16202 |
| Anatomical terms of bone | |
In humans, the sacrum (/ˈsækrəm/ or /ˈseɪkrəm/; plural: sacrums or sacra) is a large, triangular bone at the base of the spine and at the upper, back part of the pelvic cavity, where it is inserted like a wedge between the two hip bones. Its upper part connects with the last lumbar vertebra, and its lower part with the coccyx (tailbone). Usually, it begins as five unfused vertebrae which begin to fuse between the ages of 16–18 years and have usually completely fused into a single bone by the age of 34 years.
The sacrum has three different surfaces which are shaped to accommodate various structures. It articulates with four other bones. It is curved upon itself and placed obliquely (tilted forward). It is concave, facing forward. The base projects forward as the sacral promontory internally, which is the superiormost portion of the sacrum. The central part is curved outward toward the posterior, allowing greater room for the pelvic cavity. The two lateral projections of the sacrum are called the alae (wings), and articulate with the ilium at the L-shaped sacroiliac joints.
The sacral vertebrae develop by the end of the first month of embryonic development, the higher vertebrae having developed first. There are congenital disorders that develop in the early stages of the fetus.
Structure
The sacrum is a complex structure providing support for the spine and accommodation for the spinal nerves. It also articulates with the hip bones. The sacrum has three surfaces, a pelvic, dorsal and a lateral surface, a base and an apex. The base of the sacrum, which is broad and expanded, is directed upward and forward. The apex (apex ossis sacri) is directed downward, and presents an oval facet for articulation with the coccyx. The sacral canal as a continuation of the vertebral canal runs throughout the greater part of the sacrum.
Promontory
The sacral promontory marks part of the border of the pelvic inlet, and comprises the iliopectineal line and the linea terminalis.[1] The sacral promontory articulates with the last lumbar vertebra to form the sacrovertebral angle, an angle of 30 degrees from the horizontal plane that provides a useful marker for sling operation.
Surfaces


The pelvic surface of the sacrum is concave from the top, and curved slightly from side to side. Its middle part is crossed by four transverse ridges, which correspond to the original planes of separation between the five sacral vertebrae. The body of the first segment is large and has the form of a lumbar vertebra; the bodies of the next bones get progressively smaller, are flattened from the back, and curved to shape themselves to the sacrum, being concave in front and convex behind. At each end of the transverse ridges, are four anterior sacral foramina, diminishing in size in line with the smaller vertebral bodies. The foramina give exit to the anterior divisions of the sacral nerves and entrance to the lateral sacral arteries. Each part at the sides of the foramina, is traversed by four broad, shallow grooves, which lodge the anterior divisions of the sacral nerves. They are separated by prominent ridges of bone which give origin to the piriformis muscle. If a sagittal section be made through the center of the sacrum, the bodies are seen to be united at their circumferences by bone, wide intervals being left centrally, which, in the fresh state, are filled by the intervertebral discs.
The dorsal surface of the sacrum is convex and narrower than the pelvic surface. In the middle line is the middle sacral crest, surmounted by three or four tubercles; the rudimentary spinous processes of the upper three or four sacral vertebrae. On either side of the middle sacral crest is a shallow sacral groove, which gives origin to the multifidus muscle. The floor of the groove is formed by the united laminae of the corresponding vertebrae. The laminae of the fifth sacral vertebra, and sometimes those of the fourth, do not meet at the back, and thus a hiatus or deficiency occurs in the posterior wall of the sacral canal. On the lateral aspect of the sacral groove is a linear series of tubercles produced by the fusion of the articular processes which together form the indistinct sacral articular crests. The articular processes of the first sacral vertebra are large and oval shaped. Their facets are concave from side to side, face to the back and middle, and articulate with the facets on the inferior processes of the fifth lumbar vertebra. The tubercles as inferior articular processes of the fifth sacral vertebra, known as the sacral cornea, are projected downward, and are connected to the cornua of the coccyx. At the side of the articular processes are the four posterior sacral foramina; they are smaller in size and less regular in form than those at the front, and transmit the posterior divisions of the sacral nerves. On the side of the posterior sacral foramina is a series of tubercles, the transverse processes of the sacral vertebrae, and these form the lateral crests of the sacrum. The transverse tubercles of the first sacral vertebra are large and very distinct; they, together with the transverse tubercles of the second vertebra, give attachment to the horizontal parts of the posterior sacroiliac ligaments; those of the third vertebra give attachment to the oblique fasciculi of the posterior sacroiliac ligaments; and those of the fourth and fifth to the sacrotuberous ligaments.

The lateral surface of sacrum is broad above, but narrows into a thin edge below. The upper half presents in front an ear-shaped surface, the auricular surface, covered with cartilage in the immature state, for articulation with the ilium. Behind it is a rough surface, the sacral tuberosity, on which are three deep and uneven impressions, for the attachment of the posterior sacroiliac ligament. The lower half is thin, and ends in a projection called the inferior lateral angle. Medial to this angle is a notch, which is converted into a foramen by the transverse process of the first piece of the coccyx, and this transmits the anterior division of the fifth sacral nerve. The thin lower half of the lateral surface gives attachment to the sacrotuberous and sacrospinous ligaments, to some fibers of the Gluteus maximus at the back and to the Coccygeus in the front.
Articulations
The sacrum articulates with four bones:
- the last lumbar vertebra above
- the coccyx (tailbone) below
- the illium portion of the hip bone on either side
Rotation of the sacrum superiorly and anteriorly whilst the coccyx moves posteriorly relative to the ilium is sometimes called "nutation" (from the Latin term nutatio which means "nodding") and the reverse, postero-inferior motion of the sacrum relative to the ilium whilst the coccyx moves anteriorly, "counter-nutation."[2] In upright vertebrates, the sacrum is capable of slight independent movement along the sagittal plane. When you bend backward the top (base) of the sacrum moves forward relative to the ilium; when you bend forward the top moves back.[3]
The sacrum is called so when referred to all of the parts combined. Its parts are called sacral vertebrae when referred individually.
Variations
In some cases the sacrum will consist of six pieces[4] or be reduced in number to four.[5] The bodies of the first and second vertebrae may fail to unite.
Sometimes the uppermost transverse tubercles are not joined to the rest of the ala on one or both sides, or the sacral canal may be open throughout a considerable part of its length, in consequence of the imperfect development of the laminae and spinous processes.
The sacrum also varies considerably with respect to its degree of curvature.
Sexual dimorphism
The sacrum is noticeably sexually dimorphic (differently shaped in males and females).
In the female the sacrum is shorter and wider than in the male; the lower half forms a greater angle with the upper; the upper half is nearly straight, the lower half presenting the greatest amount of curvature. The bone is also directed more obliquely backward; this increases the size of the pelvic cavity and renders the sacrovertebral angle more prominent.
In the male the curvature is more evenly distributed over the whole length of the bone, and is altogether larger than in the female.
Development
The somites that give rise to the vertebral column begin to develop from head to tail along the length of the notochord. At day 20 of embryogenesis the first four pairs of somites appear in the future occipital bone region. Developing at the rate of three or four a day, the next eight pairs form in the cervical region to develop into the cervical vertebrae; the next twelve pairs will form the thoracic vertebrae; the next five pairs the lumbar vertebrae and by about day 29 the sacral somites will appear to develop into the sacral vertebrae; finally on day 30 the last three pairs will form the coccyx.[6]
Clinical significance
Congenital disorders
The congenital disorder, Spina bifida, occurs as a result of a defective embryonic neural tube, characterised by the incomplete closure of vertebral arch or of the incomplete closure of the surface of the vertebral canal.[7] The most common sites for Spina bifida malformations are the lumbar and sacral areas.
Another congenital disorder is that of caudal regression syndrome also known as sacral agenesis. This is characterised by an abnormal underdevelopment in the embryo, (occurring by the seventh week), of the lower spine.[8] Sometimes part of the coccyx is absent, or the lower vertebrae can be absent or on occasion a small part of the spine is missing with no outward sign.
In oncology
The sacrum is one of the main sites for the development of the sarcomas known as chordomas (chordosarcomas) that are derived from the remnants of the embryonic notochord.[9]
In osteopathic medicine
Sacral Diagnosis is a common issue in Osteopathic Manipulative Medicine. There are many types of sacral diagnoses, such as torsion and shear. To diagnose a sacral torsion, the axis of rotation is found with the axis named after its superior pole. If the opposite side of the pole is rotated anteriorly, it is rotated towards the pole, in which case it is called either a right-on-right (R on R) or left-on-left (L on L) torsion. The first letter in the diagnosis pertains to the direction of rotation of the superior portion of the sacrum opposite the side of the superior axis pole, and the last letter pertains to the pole.[10]
History
Etymology
The English word sacrum[7] is derived from the full Latin expression os sacrum,[11][12] a translation of Ancient Greek ἱερόν ὀστέον,[13] attested in the writings of Greek physician Galen.[13][14] Both os and ὀστέον mean bone,[14][15] and sacrum and ἱερόν mean holy or sacred.[14][15] Formerly the os sacrum was called holy bone[16] in English. In other languages similar expressions, like heiliges Bein[16] or Heiligenbein[17] (German) and heiligbeen[18] (Dutch) exist.
There are a few probable etymological explanations for ἱερόν ὀστέον. Supposedly the sacrum was the part of an animal offered in sacrifice (since the sacrum is the seat of the organs of procreation).[19] Alternatively, it was believed that that the soul of the man resided in the sacrum.[citation needed] Others[17] attribute the adjective ἱερόν to the ancient belief that this specific bone would be indestructible. Another source mentions that the os sacrum, being the largest of the vertebrae, was also called μέγας σπόνδυλος[20] by the Greeks, with μέγας, big[14] and σπόνδυλος, vertebra.[14] In certain instances ἱερός was considered as a synonym of μέγας[20] in Ancient Greek, hence the transformation from μέγας σπόνδυλος to ἱερόν ὀστέον. Latin vertebra magna,[13] with magna, big,[15] is a translation of μέγας σπόνδυλος.
Besides the aforementioned expressions, the Ancient Greeks, as attested in the poetry of Greek poet Antimachus,[14] used κλόνις,[14][21] Latinized as clonis.[21] to refer to the sacrum. Κλόνις is cognate to Latin clunis[14][21] ("buttock"[15]). The latter can be found in the genitive plural (='"of the buttocks") in the synonymous Latin expression for the ossa sacra, ossa clunium.[16] Due to the fact that the os sacrum is broad and thick at its upper end,[17] the os sacrum is alternatively called os latum,[16][20] from latum, broad.[15]
Additional images
-
Image of a female pelvis seen anteriorly, sacrum at centre.
-
Lateral surfaces of sacrum and coccyx.
-
Base of sacrum.
-
Median sagittal section of the sacrum.
-
Left Levator ani from within.
-
The posterior divisions of the sacral nerves.
-
Behind view.
-
Cut side view.
-
Lumbar and sacral plexus. Deep dissection.Anterior view.
-
Sacrum. Pelvic surface.
-
Sacrum. Dorsal surface.











See also
|
|
References
- ^ Kirschner, Celeste G. (2005). Netter's Atlas Of Human Anatomy For CPT Coding. Chicago: American medical association. p. 274. ISBN 1-57947-669-4.
- ^ Joseph D. Kurnik, DC. "The AS Ilium Fixation, Nutation, and Respect".
- ^ Maitland, J (2001). Spinal Manipulation Made Simple. Berkeley: North Atlantic Books, p. 72.
- ^ http://www.webcitation.org/query?url=http://www.geocities.com/akramjfr/sacralization.html&date=2009-10-25+12:10:24
- ^ http://www.webcitation.org/query?url=http://www.geocities.com/akramjfr/lumbarization.html&date=2009-10-25+12:10:08
- ^ Larsen, W.J. Human Embryology.2001.Churchill Livingstone Pages 63-64 ISBN 0-443-06583-7
- ^ a b Anderson, D.M. (2000). Dorland’s illustrated medical dictionary (29th edition). Philadelphia/London/Toronto/Montreal/Sydney/Tokyo: W.B. Saunders Company.
- ^ Sonek JD, Gabbe SG, Landon MB, Stempel LE, Foley MR, Shubert-Moell K (March 1990). "Antenatal diagnosis of sacral agenesis syndrome in a pregnancy complicated by diabetes mellitus". Am. J. Obstet. Gynecol. 162 (3): 806–8. PMID 2180307.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - ^ http://www.chordomafoundation.org/understanding-chordoma/
- ^ Wedel, F.P. "D.O." (PDF). A.T. Still University School of Osteopathic Medicine. Retrieved 18 February 2014.
- ^ His, W. (1895). Die anatomische Nomenclatur. Nomina Anatomica. Der von der Anatomischen Gesellschaft auf ihrer IX. Versammlung in Basel angenommenen Namen. Leipzig: Verlag Veit & Comp.
- ^ Federative Committee on Anatomical Terminology (FCAT) (1998). Terminologia Anatomica. Stuttgart: Thieme
- ^ a b c Hyrtl, J. (1880). Onomatologia Anatomica. Geschichte und Kritik der anatomischen Sprache der Gegenwart. Wien: Wilhelm Braumüller. K.K. Hof- und Unversitätsbuchhändler.
- ^ a b c d e f g h Liddell, H.G. & Scott, R. (1940). A Greek-English Lexicon. revised and augmented throughout by Sir Henry Stuart Jones. with the assistance of. Roderick McKenzie. Oxford: Clarendon Press.
- ^ a b c d e Lewis, C.T. & Short, C. (1879). A Latin dictionary founded on Andrews' edition of Freund's Latin dictionary. Oxford: Clarendon Press.
- ^ a b c d Schreger, C.H.Th.(1805). Synonymia anatomica. Synonymik der anatomischen Nomenclatur. Fürth: im Bureau für Literatur.
- ^ a b c Foster, F.D. (1891-1893). An illustrated medical dictionary. Being a dictionary of the technical terms used by writers on medicine and the collateral sciences, in the Latin, English, French, and German languages. New York: D. Appleton and Company.
- ^ Everdingen, J.J.E. van, Eerenbeemt, A.M.M. van den (2012). Pinkhof Geneeskundig woordenboek (12de druk). Houten: Bohn Stafleu Van Loghum.
- ^ Online Etymology Dictionary
- ^ a b c Hyrtl, J. (1875). Lehrbuch der Anatomie des Menschen. Mit Rücksicht auf physiologische Begründung und praktische Anwendung. (Dreizehnte Auflage). Wien: Wilhelm Braumüller K.K. Hof- und Universitätsbuchhändler.
- ^ a b c Kraus, L.A. (1844). Kritisch-etymologisches medicinisches Lexikon (Dritte Auflage). Göttingen: Verlag der Deuerlich- und Dieterichschen Buchhandlung.
External links
- Anatomy photo:43:os-0401 at the SUNY Downstate Medical Center - "The Female Pelvis: Articulated bones of pelvis"
- Anatomy photo:43:st-0401 at the SUNY Downstate Medical Center - "The Female Pelvis: Bones"
- Template:EMedicineDictionary
This article incorporates text in the public domain from page 106 of the 20th edition of Gray's Anatomy (1918)